
According to the The National Kidney Foundation�s Kidney Disease Outcomes Quality Initiative (K/DOQI) Clinical Practice Guidelines for
Vascular Access, published in year 2000, Guideline 3:
The wrist [arteriovenous] fistula is the first choice of access type because of the following advantages:
- It is simple to create.
- It preserves more proximal vessels for future access placement.
- It has few complications. Specifically, the incidence of vascular steal is low, and in mature fistulae, thrombosis and infection rates are low.
Yet Gilbert M. Gaul of WaPo notes:
Today, fewer than four in 10 dialysis patients nationwide have a fistula, despite overwhelming evidence that they are safer, cheaper and more effective than grafts and catheters.
...fistula rates remain stubbornly low in the United States, and vary dramatically by geography.
Medicare, which picks up most of the $15 billion annual tab for dialysis treatment, pays surgeons more for grafts and catheters than fistulas -- in effect, rewarding inferior care. That's because its reimbursement system is based on the time and resources needed to do a procedure, not on the outcome.
In 2003, it cost Medicare an average of $52,751 to care for a patient with a fistula, compared with $61,929 for those using a graft and $69,893 for those on a catheter, federal data show.
Patients with grafts and catheters also have a 20 to 70 percent greater chance of dying in the first year of treatment, according to CMS.
From the Rayner et al 2004 paper in the American Journal of Kidney Diseases, "Vascular access results from the Dialysis Outcomes and Practice Patterns Study (DOPPS): performance against Kidney Disease Outcomes Quality Initiative (K/DOQI) Clinical Practice Guidelines", we see that:
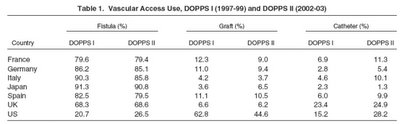
The U.S. ranks in the very bottom for fistula use in chronic hemodialysis. The DOPPS studies have produced some very interesting results. Among others, it has shown that American patients on hemodialysis have much higher mortality than those in other countries. I'm not certain if this is due to differences in patient characteristics or medical care, but it has been suggested the difference may be related to the much faster, much higher-flow hemodialysis preferred by patients and dialysis centers alike.
Technorati Tags:
Medicine / Medicare / Hemodialysis / Health policy


1 comment:
Perhaps also to note (and I apologize, as I'm too tired to read the WaPo article)--Medicare Part A reimburses catheter and graft placement, if done as an inpatient procedure. In contrast, fistula placement is often an outpatient procedure, falling under Medicare Part B, with varying reimbursement not only as described, but depending on whether patients are part of managed care plans, have cost sharing, and so on.
And an interesting artifact being that Medicare picks up most of the tab because ESRD patients automatically qualify for Medicare, regardless of age.
Post a Comment